- Record: found
- Abstract: found
- Article: found
Reducing the Delay Between Stroke Onset and Hospital Arrival: Is It an Achievable Goal?
editorial
Read this article at
There is no author summary for this article yet. Authors can add summaries to their articles on ScienceOpen to make them more accessible to a non-specialist audience.
Abstract
In this issue of the Journal of the American Heart Association (JAHA), Addo and colleagues
1
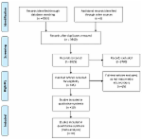
report on prehospital delay by using data from the South London Stroke Registry, a
high-quality population-based acute stroke registry that collected data on more than
2000 first-time stroke events over a 9-year period between 2002 and 2010. Among the
subset of 1392 out-of-hospital stroke events for which stroke onset-to-arrival (OTA)
time data were available, the study found that almost 40% of cases arrived at 1 of
the 5 registry hospitals within 3 hours of onset and that the overall median OTA time
was 4.7 (interquartile range, 1.5 to 12.7) hours. Unfortunately, data were not presented
by study year (ie, 2002 through 2010) to determine if there was any secular improvement
in OTA times over this time period. Commendably, 11% of the 1085 ischemic stroke admissions
in this study were treated with thrombolysis. In a multivariable logistic regression
analysis of prehospital delay (defined as OTA >3 hours), the authors found that black
ethnicity, living alone, and nighttime stroke onset were all associated with increased
delay, whereas stroke severity was strongly associated with lower odds of delayed
arrival. A further multivariable analysis of thrombolysis treatment was undertaken
among all 1085 ischemic stroke admissions; the results identified age, ethnicity,
and nighttime stroke onset as significant predictors, along with higher stroke severity,
which was very strongly related to thrombolysis treatment (presumably because of its
direct effects on OTA time). The study also reported on the impact of a 1-year national
education campaign (based on the F.A.S.T. [face, arms, speech, and time] stroke assessment
criteria) designed to educate the public on stroke signs and symptoms and the benefits
of rapid treatment. There was no detectable effect of this campaign on OTA times or
thrombolysis treatment.
Given the unique urban location and high-quality methods used in this registry, it
is interesting to compare and contrast the findings of this study with the many other
previous reports that have covered a diverse range of populations and time periods.
The 40% of subjects who arrived within 3 hours and the median OTA time of a little
less than 5 hours are well within the range previously reported in a systematic review.
2
The observation that greater stroke severity was associated with shorter prehospital
delay, while stroke onset at night was associated with longer delay is also consistent
with previous studies.
3
Surprisingly, the majority of studies examining the impact of living alone on prehospital
delay among stroke patients have shown that living alone is not associated with longer
OTA times,
3
so the finding by Addo and colleagues that living alone was associated with longer
delays is an important observation, as is the fact that black patients had longer
prehospital delays.
Despite the registry's high level of organization and maturity, it is also important
to note that OTA times could not be calculated in 22% (n =454) of the cases. Although
there were limited differences in demographic characteristics when cases with missing
OTA data were compared to those with OTA data, the fact that stroke severity was markedly
lower in the cases with missing OTA data suggests that the registry hospitals did
not bother to record onset or arrival times in these patients, either because they
had mild or resolving symptoms on arrival or because they had arrived well after the
therapeutic window for acute stroke treatment. A recent Get With The Guidelines (GWTG)—Stroke
study from the United States examined trends in OTA times and found that 53% of ischemic
stroke admissions did not have a documented OTA time.
4
The cases with missing OTA times had mostly mild symptoms and in all likelihood also
arrived after the time window for acute stroke treatments. The point to emphasize
here is that having a substantial proportion of patients with missing OTA data, even
in high-quality studies such as the South London Stroke Registry, negatively affects
our ability to make inferences about the underlying trends and causes of delayed arrival.
5
Given the limited success of prior mass educational campaigns on reducing OTA times
or improving thrombolysis treatment rates,
6
it is perhaps not surprising that the education campaign described by Addo and colleagues
had no statistically significant impact on these 2 outcomes. Although it is clear
that education campaigns can improve the public's knowledge and understanding of stroke
signs and symptoms, as well as the need for emergency care,
7,8
their effects on hard clinical outcomes such as arrival times and thrombolysis treatment
rates have been unequivocally disappointing.
6
It has become increasingly evident that for stroke education campaigns to have any
chance of being effective, we need to focus on the disconnect between stroke knowledge
and actions. Specifically, we need to understand why stroke patients and their bystanders
delay calling emergency medical services.
3,6
Numerous studies have demonstrated that, contrary to the commonly held premise, increased
knowledge of stroke does not translate to an increase in appropriate actions.
9–11
For public education campaigns to have any hope of modifying OTA times, it is important
that they directly increase the motivation to call emergency medical services (9-1-1)
quickly. This should be done by targeting outcome expectations, improving stroke recognition
skills, and addressing community norms.
3,10
To increase the motivation to call 9-1-1 immediately after recognizing stroke symptoms,
the public must come to believe that acting rapidly will result in better outcomes
and that perceived barriers to calling 9-1-1 (such as financial costs and embarrassment)
have been removed. Educational efforts should motivate the public to respond quickly
to stroke symptoms by connecting rapid response to improved health outcomes. Before
investing further public resources in mass education efforts around stroke, we need
to return to the drawing board and obtain a much better understanding of the facilitators
of and barriers to early and aggressive action among the general public. This greater
understanding then needs to inform the development of new educational methods and
messages that should be developed with the use of theory-grounded principles and tested
with solid evidence-based evaluation methods.
6
In the absence of these renewed efforts, one wonders if meaningful reductions in the
delay between stroke onset and hospital arrival will ever be achievable.
Related collections
Most cited references6
- Record: found
- Abstract: found
- Article: found
Systematic review of mass media interventions designed to improve public recognition of stroke symptoms, emergency response and early treatment
Jan Lecouturier, Helen Rodgers, Madeleine Murtagh … (2010)
- Record: found
- Abstract: found
- Article: not found
Lack of association between stroke symptom knowledge and intent to call 911: a population-based survey.
Lewis Morgenstern, Chris Fussman, Sarah Lyon-Callo … (2010)
- Record: found
- Abstract: found
- Article: found
Changes in Knowledge of Stroke Risk Factors and Warning Signs among Michigan Adults
Mathew Reeves, Ann Rafferty, Alison A.R. Aranha … (2008)