- Record: found
- Abstract: found
- Article: found
Prehospital paths and hospital arrival time of patients with acute coronary syndrome or stroke, a prospective observational study

Read this article at
Abstract
Background
Patients with a presumed diagnosis of acute coronary syndrome (ACS) or stroke may have had contact with several healthcare providers prior to hospital arrival. The aim of this study was to describe the various prehospital paths and the effect on time delays of patients with ACS or stroke.
Methods
This prospective observational study included patients with presumed ACS or stroke who may choose to contact four different types of health care providers. Questionnaires were completed by patients, general practitioners (GP), GP cooperatives, ambulance services and emergency departments (ED). Additional data were retrieved from hospital registries.
Results
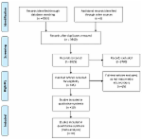
Two hundred two ACS patients arrived at the hospital by 15 different paths and 243 stroke patients by ten different paths. Often several healthcare providers were involved (60.8 % ACS, 95.1 % stroke). Almost half of all patients first contacted their GP (47.5 % ACS, 49.4 % stroke). Some prehospital paths were more frequently used, e.g. GP (cooperative) and ambulance in ACS, and GP or ambulance and ED in stroke. In 65 % of all events an ambulance was involved. Median time between start of symptoms and hospital arrival for ACS patients was over 6 h and for stroke patients 4 h. Of ACS patients 47.7 % waited more than 4 h before seeking medical advice compared to 31.6 % of stroke patients. Median time between seeking medical advice to arrival at hospital was shortest in paths involving the ambulance only (60 min ACS, 54 min stroke) or in combination with another healthcare provider (80 to 100 min ACS, 99 to 106 min stroke).
Conclusions
Prehospital paths through which patients arrived in hospital are numerous and often complex, and various time delays occurred. Delays depend on the entry point of the health care system, and dialing the emergency number seems to be the best choice. Since reducing patient delay is difficult and noticeable differences exist between various prehospital paths, further research into reasons for these different entry choices may yield possibilities to optimize paths and reduce overall time delay.
Related collections
Most cited references21
- Record: found
- Abstract: found
- Article: not found
Streamlining of prehospital stroke management: the golden hour.
- Record: found
- Abstract: found
- Article: not found
A comprehensive review of prehospital and in-hospital delay times in acute stroke care.
- Record: found
- Abstract: found
- Article: found