- Record: found
- Abstract: found
- Article: not found
Modeling and simulations of CoViD-19 molecular mechanism induced by cytokines storm during SARS-CoV2 infection

Read this article at

Abstract
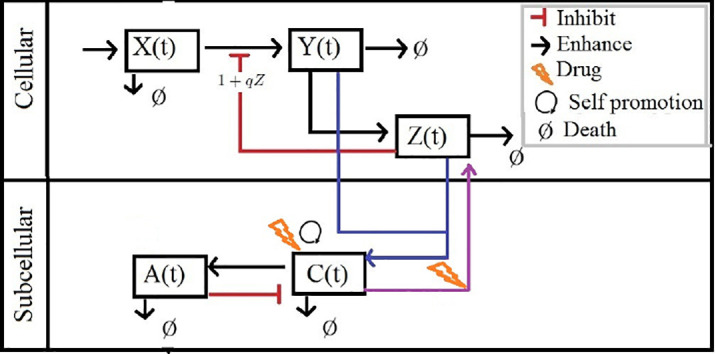
It is highly desired to explore the interventions of COVID-19 for early treatment strategies. Such interventions are still under consideration. A model is benchmarked research and comprises target cells, virus infected cells, immune cells, pro-inflammatory cytokines, and, anti-inflammatory cytokine. The interaction of the drug with the inflammatory sub-system is analyzed with the aid of kinetic modeling. The impact of drug therapy on the immune cells is modelled and the computational framework is verified with the aid of numerical simulations. The work includes a significant hypothesis that quantifies the complex dynamics of the infection, by relating it to the effect of the inflammatory syndrome generated by IL-6. In this paper we use the cancer immunoediting process: a dynamic process initiated by cancer cells in response to immune surveillance of the immune system that it can be conceptualized by an alternating movement that balances immune protection with immune evasion. The mechanisms of resistance to immunotherapy seem to broadly overlap with those used by cancers as they undergo immunoediting to evade detection by the immune system. In this process the immune system can both constrain and promote tumour development, which proceeds through three phases termed: (i) Elimination, (ii) Equilibrium, and, (iii) Escape [ 1]. We can also apply these concepts to viral infection, which, although it is not exactly “immunoediting”, has many points in common and helps to understand how it expands into an “untreated” host and can help in understanding the SARS-CoV2 virus infection and treatment model.
Graphical abstract
Highlights
Related collections
Most cited references29
- Record: found
- Abstract: found
- Article: found
COVID-19: consider cytokine storm syndromes and immunosuppression

- Record: found
- Abstract: found
- Article: found
Structural basis for the recognition of SARS-CoV-2 by full-length human ACE2
- Record: found
- Abstract: found
- Article: not found