- Record: found
- Abstract: found
- Article: found
Mental Health–Related Emergency Department Visits Among Children Aged <18 Years During the COVID-19 Pandemic — United States, January 1–October 17, 2020
research-article

Rebecca T. Leeb , PhD
1
,
,
Rebecca H. Bitsko , PhD
1 ,
Lakshmi Radhakrishnan , MPH
2 ,
Pedro Martinez , MPH
3 ,
Rashid Njai , PhD
4 ,
Kristin M. Holland , PhD
5
13 November 2020
Read this article at
There is no author summary for this article yet. Authors can add summaries to their articles on ScienceOpen to make them more accessible to a non-specialist audience.
Abstract
Published reports suggest that the coronavirus disease 2019 (COVID-19) pandemic has
had a negative effect on children’s mental health (
1
,
2
). Emergency departments (EDs) are often the first point of care for children experiencing
mental health emergencies, particularly when other services are inaccessible or unavailable
(
3
). During March 29–April 25, 2020, when widespread shelter-in-place orders were in
effect, ED visits for persons of all ages declined 42% compared with the same period
in 2019; during this time, ED visits for injury and non-COVID-19–related diagnoses
decreased, while ED visits for psychosocial factors increased (
4
). To assess changes in mental health–related ED visits among U.S. children aged <18
years, data from CDC’s National Syndromic Surveillance Program (NSSP) from January
1 through October 17, 2020, were compared with those collected during the same period
in 2019. During weeks 1–11 (January 1–March 15, 2020), the average reported number
of children’s mental health–related ED visits overall was higher in 2020 than in 2019,
whereas the proportion of children’s mental health–related visits was similar. Beginning
in week 12 (March 16) the number of mental health–related ED visits among children
decreased 43% concurrent with the widespread implementation of COVID-19 mitigation
measures; simultaneously, the proportion of mental health–related ED visits increased
sharply beginning in mid-March 2020 (week 12) and continued into October (week 42)
with increases of 24% among children aged 5–11 years and 31% among adolescents aged
12–17 years, compared with the same period in 2019. The increased proportion of children’s
mental health–related ED visits during March–October 2020 might be artefactually inflated
as a consequence of the substantial decrease in overall ED visits during the same
period and variation in the number of EDs reporting to NSSP. However, these findings
provide initial insight into children’s mental health in the context of the COVID-19
pandemic and highlight the importance of continued monitoring of children’s mental
health throughout the pandemic, ensuring access to care during public health crises,
and improving healthy coping strategies and resiliency among children and families.
CDC analyzed NSSP ED visit data, which include a subset of hospitals in 47 states
representing approximately 73% of U.S. ED visits.* Mental health–related ED visits
among children aged <18 years was a composite variable derived from the mental health
syndrome query of the NSSP data for conditions likely to result in ED visits during
and after disaster events (e.g., stress, anxiety, acute posttraumatic stress disorder,
and panic).
†
Weekly numbers of mental health–related ED visits and proportions of mental health–related
ED visits (per 100,000 pediatric ED visits
§
) were computed overall, stratified by age group (0–4, 5–11, and 12–17 years) and
sex, and compared descriptively with the corresponding weekly numbers and proportions
for 2019. Numbers and proportions of visits were compared during calendar weeks 1–11
(January 1–March 14, 2020) and weeks 12–42 (March 15–October 17, 2020) (before and
after a distinct decrease in overall ED visits reported beginning in week 12 in 2020)
¶
(
4
). Analyses are descriptive and statistical comparisons were not performed.
The number of children’s mental health–related ED visits decreased sharply from mid-March
2020 (week 12, March 15–21) through early April (week 15, April 5–11) and then increased
steadily through October 2020. (Figure 1). During the same time, the overall proportion
of reported children’s ED visits for mental health–related concerns increased and
remained higher through the end of the reporting period in 2020 than that in 2019
(Figure 1). The proportion of mental health–related ED visits among children increased
66%, from 1,094 per 100,000 during April 14–21, 2019 to 1,820 per 100,000 during April
12–18, 2020 (Supplementary Figure 1, https://stacks.cdc.gov/view/cdc/96609). Although
the average reported number of children’s mental health–related ED visits overall
was 25% higher during weeks 1–11 in 2020 (342,740) than during the corresponding period
in 2019 (274,736), the proportion of children’s mental health–related visits during
the same time was similar (1,162 per 100,000 in 2020 versus 1,044 per 100,000 in 2019).
(Table). During weeks 12–42, 2020 (mid-March–October) however, average weekly reported
numbers of total ED visits by children were 43% lower (149,055), compared with those
during 2019 (262,714), whereas the average proportion of children’s mental health–related
ED visits was approximately 44% higher in 2020 (1,673 per 100,000) than that in 2019
(1,161 per 100,000).
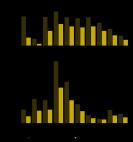
FIGURE 1
Weekly number of emergency department (ED) mental health–related visits (A) and proportion
of (B) children’s mental health–related ED visits per total ED visits* among children
aged <18 years — National Syndromic Surveillance Program, United States, January–October
2019 and 2020
* Proportion of mental health–related ED visits = number of ED visits for children’s
mental health/total number of pediatric ED visits x 100,000.
The figure is a line chart showing the weekly number of emergency department (ED)
mental health–related visits (A) and proportion of (B) children’s mental health–related
ED visits per total ED visits among children aged <18 years, using data from the National
Syndromic Surveillance Program, in the United States, during January–October 2019
and 2020.
TABLE
Average number and proportions* of emergency department (ED) visits and mental health–related
ED visits
†
among children aged <18 years — National Syndromic Surveillance Program (NSSP), United
States, 2019–2020
Surveillance period/indicators
2019
2020
Age group, yrs
Age group, yrs
All <18
0–4
5–11
12–17
All <18
0–4
5–11
12–17
Weeks 1–42
§
Average weekly total ED visits
265,863
110,002
81,133
74,728
199,782
78,742
59,660
61,380
Average weekly mental health–related ED visits
3,025
80
625
2,320
2,872
54
522
2,296
Mental health–related ED visits per 100,000 visits
1,130
73
762
3,084
1,539
75
919
3,863
Weeks 1–11
¶
Average weekly total ED visits
274,736
118,926
83,924
71,886
342,740
143,789
107,049
91,902
Average weekly mental health–related ED visits
2,876
82
594
2,200
3,974
80
821
3,073
Mental health–related ED visits per 100,000 visits
1,044
69
707
30,45
1,162
56
769
3,333
Weeks 12–42**
Average weekly total ED visits
262,714
106,835
80,143
75,736
149,055
55,661
42,844
50,550
Average weekly mental health–related ED visits
3,078
79
635
2,363
2,481
45
416
2,020
Mental health–related ED visits per 100,000 visits
1,161
75
782
3,098
1,673
81
972
4,051
* Average proportion of ED visits for children’s mental health = (average number of
ED visits for children’s mental health/average total number of ED visits for the same
age or sex population [e.g., children aged 18 years]) x 100,000. All numbers have
been rounded to the nearest whole number.
† Mental health–related ED visits were defined using NSSP’s Syndrome Definition (SD)
Subcommittee community-developed syndrome definition for mental health conditions
likely to increase in ED frequency during and after natural or human-caused disaster
events. This syndrome definition attempts to leverage only mental health conditions
and presentations that showed increases in visit frequency after select disasters
in the United States. There are no disaster-related terms inherent to this query.
The query has been added to NSSP BioSense Platform Electronic Surveillance System
for the Early Notification of Community-based Epidemics as a Chief Complaint and Discharge
Diagnosis category. https://knowledgerepository.syndromicsurveillance.org/disaster-related-mental-health-v1-syndrome-definition-subcommittee.
§ Weeks 1–42 in 2019 correspond to December 30, 2018–October 19, 2019; weeks 1–42
in 2020 correspond to December 29, 2019–October 17, 2020.
¶ Weeks 1–11 in 2019 correspond to December 30, 2018–March 16, 2019; weeks 1–11 in
2020 correspond to December 29, 2019–March 14, 2020.
** Weeks 12–42 in 2019 correspond to March 17–October 19, 2019; weeks 12–42 in 2020
correspond to March 15–October 17, 2020.
Adolescents aged 12–17 years accounted for the largest proportion of children’s mental
health–related ED visits during 2019 and 2020 (Figure 2). During weeks 12–42, 2020,
the proportion of mental health–related visits for children aged 5–11 years and adolescents
aged 12–17 years increased approximately 24% and 31%, respectively compared with those
in 2019; the proportion of mental health–related visits for children aged 0–4 years
remained similar in 2020. (Table.) The highest weekly proportion of mental health–related
ED visits occurred during October for children aged 5–11 years (week 42; 1,177 per
100,000) and during April (week 16) for adolescents aged 12–17 years (4,758 per 100,000)
(Figure 2).
FIGURE 2
Weekly proportion of mental health–related emergency department (ED) visits* per total
ED visits among children aged <18 years, by age group — National Syndromic Surveillance
Program, United States, January–October 2019 and 2020
* Proportion of mental health–related ED visits = number of ED visits for children’s
mental health/total number of pediatric ED visits x 100,000.
The figure is a line chart showing the weekly proportion of mental health–related
emergency department (ED) visits per total ED visits among children aged <18 years,
by age group, using data from the National Syndromic Surveillance Program, in the
United States, during January–October 2019 and 2020.
During 2019 and 2020, the proportion of mental health–related ED visits was higher
among females aged <18 years than it was among males (Supplementary Figure 2, https://stacks.cdc.gov/view/cdc/96610).
Similar patterns of increasing proportions of mental health–related ED visits were
observed in 2020 for males and females, with increases beginning mid-March and continuing
through October.
Discussion
Substantial declines in the overall reported numbers of children’s mental health–related
ED visits occurred in 2020 during mid-March to early May, coincident with the widespread
implementation of community mitigation measures** enacted to prevent COVID-19 transmission
(e.g., school closures and restrictions to nonemergent care) and decreases in overall
ED visits for the same period (
4
). A previous report found the mean weekly number of ED visits for children aged <14
years declined approximately 70% during March 29–April 25, 2020, relative to the corresponding
period in 2019 (
4
). Further, the mean number of weekly ED visits for persons of all ages decreased
significantly for asthma (–10%), otitis media (–65%), and sprain- and strain-related
injuries (–39%), and mean weekly ED visits for psychosocial factors increased 69%
(
4
). This report demonstrates that, whereas the overall number of children’s mental
health–related ED visits decreased, the proportion of all ED visits for children’s
mental health–related concerns increased, reaching levels substantially higher beginning
in late-March to October 2020 than those during the same period during 2019. Describing
both the number and the proportion of mental health–related ED visits provides crucial
context for these findings and suggests that children’s mental health warranted sufficient
concern to visit EDs during a time when nonemergent ED visits were discouraged.
Many children receive mental health services through clinical and community agencies,
including schools (
5
). The increase in the proportion of ED visits for children’s mental health concerns
might reflect increased pandemic-related stress and unintended consequences of mitigation
measures, which reduced or modified access to children’s mental health services (
2
), and could result in increased reliance on ED services for both routine and crisis
treatment (
3
). However, the magnitude of the increase should be interpreted carefully because
it might also reflect the large decrease in the number and proportion of other types
of ED visits (e.g., asthma, otitis media, and musculoskeletal injuries) (
4
) and variation in the number of EDs reporting to NSSP.
Adolescents aged 12–17 years accounted for the highest proportion of mental health–related
ED visits in both 2019 and 2020, followed by children aged 5–11 years. Many mental
disorders commence in childhood, and mental health concerns in these age groups might
be exacerbated by stress related to the pandemic and abrupt disruptions to daily life
associated with mitigation efforts, including anxiety about illness, social isolation,
and interrupted connectedness to school (
5
). The majority of EDs lack adequate capacity to treat pediatric mental health concerns
(
6
), potentially increasing demand on systems already stressed by the COVID-19 pandemic.
These findings demonstrate continued need for mental health care for children during
the pandemic and highlight the importance of expanding mental health services, such
as telemental health and technology-based solutions (e.g., mobile mental health applications)
(
5
,
7
).
The findings in this report are subject to at least three limitations. First, the
proportions presented should be interpreted with caution because of variations affecting
the denominators used to calculate proportions. Children’s mental health–related ED
visits constitute a small percentage of all pediatric ED visits (1.1% in 2019 and
1.4% in 2020), increasing susceptibility of rates to decreases in ED visits during
the pandemic. In addition, NSSP ED participation can vary over time; however, analyzing
number of visits and proportion of total ED visits provides context for observed variation.
Second, NSSP data are not nationally representative; these findings might not be generalizable
beyond those EDs participating in NSSP. Further, usable information on race and ethnicity
was not available in the NSSP data. Finally, these data are subject to under- and
overestimation. Variation in reporting and coding practices can influence the number
and proportion of mental health–related visits observed. ED visits represent unique
events, not individual persons, and as such, might reflect multiple visits for one
person. The definition of mental health focuses on symptoms and conditions (e.g.,
stress, anxiety) that might increase after a disaster in the United States and might
not reflect all mental health–related ED visits. Still, these data likely underestimate
the actual number of mental health–related health care visits because many mental
health visits occur outside of EDs.
Children’s mental health during public health emergencies can have both short- and
long-term consequences to their overall health and well-being (
8
). This report provides timely surveillance data concerning children’s mental health
in the context of the COVID-19 pandemic. Ongoing collection of a broad range of children’s
mental health data outside the ED is needed to monitor the impact of COVID-19 and
the effects of public health emergencies on children’s mental health. Ensuring availability
of and access to developmentally appropriate mental health services for children outside
the in-person ED setting will be important as communities adjust mitigation strategies
(
3
). Implementation of technology-based, remote mental health services and prevention
activities to enhance healthy coping and resilience in children might effectively
support their well-being throughout response and recovery periods (
5
,
7
). CDC supports efforts to promote the emotional well-being of children and families
and provides developmentally appropriate resources for families to reduce stressors
that might contribute to children’s mental health–related ED visits
††
(
9
).
Summary
What is already known about this topic?
Emergency departments (EDs) are often the first point of care for children’s mental
health emergencies. U.S. ED visits for persons of all ages declined during the early
COVID-19 pandemic (March–April 2020).
What is added by this report?
Beginning in April 2020, the proportion of children’s mental health–related ED visits
among all pediatric ED visits increased and remained elevated through October. Compared
with 2019, the proportion of mental health–related visits for children aged 5–11 and
12–17 years increased approximately 24%. and 31%, respectively.
What are the implications for public health practice?
Monitoring indicators of children's mental health, promoting coping and resilience,
and expanding access to services to support children's mental health are critical
during the COVID-19 pandemic.
Related collections
Most cited references6
- Record: found
- Abstract: found
- Article: found
Impact of the COVID-19 Pandemic on Emergency Department Visits — United States, January 1, 2019–May 30, 2020
- Record: found
- Abstract: not found
- Article: not found
Coronavirus Disease 2019 (COVID-19) and Mental Health for Children and Adolescents
Ezra Golberstein, Hefei Wen, Benjamin F. Miller (2020)
- Record: found
- Abstract: found
- Article: not found