- Record: found
- Abstract: found
- Article: not found
A systematic review and meta-analysis of published research data on COVID-19 infection-fatality rates
Read this article at

Highlights
-
•
COVID-19 infection-fatality rate (IFR) is an important statistic for policy about the disease.
-
•
Published estimates vary, with a ‘true’ fatality rate hard to calculate.
-
•
Systematically reviewing the literature and meta-analyzing the results shows an IFR of 0.68% (0.53-0.82%).
-
•
This rate was variable from place to place, with a lower range of 0.17% and a highest estimate of 1.7%.
-
•
Serology studies with a lower risk of bias appeared to demonstrate a higher IFR than those at a higher risk of bias.
Abstract
An important unknown during the COVID-19 pandemic has been the infection-fatality rate (IFR). This differs from the case-fatality rate (CFR) as an estimate of the number of deaths as a proportion of the total number of cases, including those who are mild and asymptomatic. While the CFR is extremely valuable for experts, IFR is increasingly being called for by policy-makers and the lay public as an estimate of the overall mortality from COVID-19.
Methods
Pubmed, Medline, SSRN, and Medrxiv were searched using a set of terms and Boolean operators on 25/04/2020 and re-searched 14/05/2020, 21/05/2020, and 16/06/2020. Articles were screened for inclusion by both authors. Meta-analysis was performed in Stata 15.1 using the metan command, based on IFR and confidence intervals extracted from each study. Google/Google Scholar was used to assess the grey literature relating to government reports.
Results
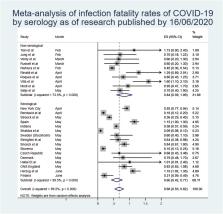
After exclusions, there were 24 estimates of IFR included in the final meta-analysis, from a wide range of countries, published between February and June 2020.
The meta-analysis demonstrated a point-estimate of IFR of 0.68% (0.53-0.82%) with high heterogeneity (p < 0.001).
Conclusion
Based on a systematic review and meta-analysis of published evidence on COVID-19 until July, 2020, the IFR of the disease across populations is 0.68% (0.53-0.82%). However, due to very high heterogeneity in the meta-analysis, it is difficult to know if this represents a wholly unbiased point estimate. It is likely that, due to age and perhaps underlying comorbidities in the population, different places will experience different IFRs due to the disease. Given issues with mortality recording, it is also likely that this represents an underestimate of the true IFR figure. More research looking at age-stratified IFR is urgently needed to inform policy-making on this front.
Related collections
Most cited references54
- Record: found
- Abstract: found
- Article: not found
An interactive web-based dashboard to track COVID-19 in real time
- Record: found
- Abstract: found
- Article: not found
The epidemiology and pathogenesis of coronavirus disease (COVID-19) outbreak
- Record: found
- Abstract: found
- Article: found