- Record: found
- Abstract: found
- Article: found
Health care provider practices in diagnosis and treatment of malaria in rural communities in Kisumu County, Kenya
Read this article at
Abstract
Background
Accurate malaria diagnosis and appropriate treatment at local health facilities are critical to reducing morbidity and human reservoir of infectious gametocytes. The current study assessed the accuracy of malaria diagnosis and treatment practices in three health care facilities in rural western Kenya.
Methods
The accuracy of malaria detection and treatment recommended compliance was monitored in two public and one private hospital from November 2019 through March 2020. Blood smears from febrile patients were examined by hospital laboratory technicians and re-examined by an expert microscopists thereafter subjected to real-time polymerase chain reaction (RT-PCR) for quality assurance. In addition, blood smears from patients diagnosed with malaria rapid diagnostic tests (RDT) and presumptively treated with anti-malarial were re-examined by an expert microscopist.
Results
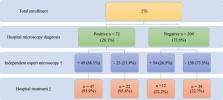
A total of 1131 febrile outpatients were assessed for slide positivity (936), RDT (126) and presumptive diagnosis (69). The overall positivity rate for Plasmodium falciparum was 28% (257/936). The odds of slide positivity was higher in public hospitals, 30% (186/624, OR:1.44, 95% CI = 1.05–1.98, p < 0.05) than the private hospital 23% (71/312, OR:0.69, 95% CI = 0.51–0.95, p < 0.05). Anti-malarial treatment was dispensed more at public hospitals (95.2%, 177/186) than the private hospital (78.9%, 56/71, p < 0.0001). Inappropriate anti-malarial treatment, i.e. artemether-lumefantrine given to blood smear negative patients was higher at public hospitals (14.6%, 64/438) than the private hospital (7.1%, 17/241) ( p = 0.004). RDT was the most sensitive (73.8%, 95% CI = 39.5–57.4) and specific (89.2%, 95% CI = 78.5–95.2) followed by hospital microscopy (sensitivity 47.6%, 95% CI = 38.2–57.1) and specificity (86.7%, 95% CI = 80.8–91.0). Presumptive diagnosis had the lowest sensitivity (25.7%, 95% CI = 13.1–43.6) and specificity (75.0%, 95% CI = 50.6–90.4). RDT had the highest non-treatment of negatives [98.3% (57/58)] while hospital microscopy had the lowest [77.3% (116/150)]. Health facilities misdiagnosis was at 27.9% (77/276). PCR confirmed 5.2% (4/23) of the 77 misdiagnosed cases as false positive and 68.5% (37/54) as false negative.
Conclusions
The disparity in malaria diagnosis at health facilities with many slide positives reported as negatives and high presumptive treatment of slide negative cases, necessitates augmenting microscopic with RDTs and calls for Ministry of Health strengthening supportive infrastructure to be in compliance with treatment guidelines of Test, Treat, and Track to improve malaria case management.
Related collections
Most cited references44
- Record: found
- Abstract: found
- Article: not found
Epidemiology and infectivity of Plasmodium falciparum and Plasmodium vivax gametocytes in relation to malaria control and elimination.
- Record: found
- Abstract: found
- Article: not found
Malaria misdiagnosis: effects on the poor and vulnerable.
- Record: found
- Abstract: found
- Article: found