- Record: found
- Abstract: found
- Article: found
Trends in Suicide Among Youth Aged 10 to 19 Years in the United States, 1975 to 2016
Read this article at
Key Points
Question
Does the disproportionate increase in suicide rates among female youth indicate a narrowing of the historically large gap between male and female youth in suicide?
Findings
This cross-sectional study of 85 051 youth suicide deaths found a significant reduction in the gap between male and female rates of suicide among youth aged 10 to 19 in the United States, with the most pronounced narrowing in younger individuals. Female suicide rates by hanging or suffocation are approaching those of male youth, and significant differences by race/ethnicity also exist.
Abstract
This cross-sectional study investigates trends in suicide rates among US youth aged 10 to 19 years by sex, age group, race/ethnicity, and method of suicide.
Abstract
Importance
Suicide is a leading cause of death among youth aged 10 to 19 years in the United States, with rates traditionally higher in male than in female youth. Recent national mortality data suggest this gap may be narrowing, which warrants investigation.
Objective
To investigate trends in suicide rates among US youth aged 10 to 19 years by age group, sex, race/ethnicity, and method of suicide.
Design, Setting, and Participants
Cross-sectional study using period trend analysis of US suicide decedents aged 10 to 19 years from January 1, 1975, to December 31, 2016. Data were analyzed for periods defined by statistically significant changes in suicide rate trends. Suicide rates were calculated using population estimates.
Main Outcomes and Measures
Period trends in suicide rates by sex and age group were assessed using joinpoint regression. Incidence rate ratios (IRRs) were estimated using negative binomial regression comparing male and female suicide rates within periods.
Results
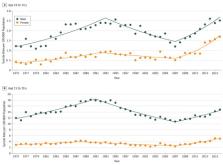
From 1975 to 2016, we identified 85 051 youth suicide deaths in the United States (68 085 male [80.1%] and 16 966 female [19.9%]) with a male to female IRR of 3.82 (95% CI, 3.35-4.35). Following a downward trend until 2007, suicide rates for female youth showed the largest significant percentage increase compared with male youth (12.7% vs 7.1% for individuals aged 10-14 years; 7.9% vs 3.5% for individuals aged 15-19 years). The male to female IRR decreased significantly across the study period for youth aged 10 to 14 years (3.14 [95% CI, 2.74-3.61] to 1.80 [95% CI, 1.53-2.12]) and 15 to 19 years (4.15 [95% CI, 3.79-4.54] to 3.31 [95% CI, 2.96-3.69]). Significant declining trends in the male to female IRR were found in non-Hispanic white youth aged 10 to 14 years (3.27 [95% CI, 2.68-4.00] to 2.04 [95% CI, 1.45-2.89]) and non-Hispanic youth of other races aged 15 to 19 years (4.02 [95% CI, 3.29-4.92] to 2.35 [95% CI, 2.00-2.76]). The male to female IRR for firearms increased significantly for youth aged 15 to 19 years (χ 2 = 7.74; P = .02 for sex × period interaction). The male to female IRR of suicide by hanging or suffocation decreased significantly for both age groups (10-14 years: χ 2 = 88.83; P < .001 for sex × period interaction and 15-19 years: χ 2 = 82.15; P < .001 for sex × period interaction). No significant change was found in the male to female IRR of suicide by poisoning across the study period.
Conclusions and Relevance
A significant reduction in the historically large gap in youth suicide rates between male and female individuals underscores the importance of interventions that consider unique differences by sex. Future research examining sex-specific factors associated with youth suicide is warranted.
Related collections
Most cited references14

- Record: found
- Abstract: found
- Article: found
Youth Risk Behavior Surveillance — United States, 2017
- Record: found
- Abstract: found
- Article: not found
Adolescent suicide and suicidal behavior.
- Record: found
- Abstract: found
- Article: not found