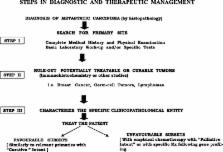
Metastatic Cancer of Unknown Primary Site (CUP) accounts for approximately 3% of all malignant neoplasms and is therefore one of the 10 most frequent cancer diagnoses in man. Patients with CUP present with metastatic disease for which the site of origin cannot be identified at the time of diagnosis. It is now accepted that CUP represents a heterogeneous group of malignancies that share a unique clinical behaviour and, presumably, unique biology. The following clinicopathological entities have been recognised: (i) metastatic CUP primarily to the liver or to multiple sites, (ii) metastatic CUP to lymph nodes including the sub-sets involving primarily the mediastinal-retroperitoneal, the axillary, the cervical or the inguinal nodes, (iii) metastatic CUP of peritoneal cavity including the peritoneal papillary serous carcinomatosis in females and the peritoneal non-papillary carcinomatosis in males or females, (iv) metastatic CUP to the lungs with parenchymal metastases or isolated malignant pleural effusion, (v) metastatic CUP to the bones, (vi) metastatic CUP to the brain, (vii) metastatic neuroendocrine carcinomas and (viii) metastatic melanoma of an unknown primary. Extensive work-up with specific pathology investigations (immunohistochemistry, electron microscopy, molecular diagnosis) and modern imaging technology (computed tomography (CT), mammography, Positron Emission Tomography (PET) scan) have resulted in some improvements in diagnosis; however, the primary site remains unknown in most patients, even on autopsy. The most frequently detected primaries are carcinomas hidden in the lung or pancreas. Several favourable sub-sets of CUP have been identified, which are responsive to systemic chemotherapy and/or locoregional treatment. Identification and treatment of these patients is of paramount importance. The considered responsive sub-sets to platinum-based chemotherapy are the poorly differentiated carcinomas involving the mediastinal-retroperitoneal nodes, the peritoneal papillary serous adenocarcinomatosis in females and the poorly differentiated neuroendocrine carcinomas. Other tumours successfully managed by locoregional treatment with surgery and/or irradiation are the metastatic adenocarcinoma of isolated axillary nodes, metastatic squamous cell carcinoma of cervical nodes, or any other single metastatic site. Empirical chemotherapy benefits some of the patients who do not fit into any favourable sub-set, and should be considered in patients with a good performance status.