- Record: found
- Abstract: found
- Article: found
Clinical Frailty Scale in an Acute Medicine Unit: a Simple Tool That Predicts Length of Stay
Read this article at
Abstract
Background
Frailty is characterized by increased vulnerability to external stressors. When frail older adults are admitted to hospital, they are at increased risk of adverse events including falls, delirium, and disability. The Clinical Frailty Scale (CFS) is a practical and efficient tool for assessing frailty; however, its ability to predict outcomes has not been well studied within the acute medical service.
Objective
To examine the CFS in elderly patients admitted to the acute medical ward and its association with length of stay.
Design
Prospective cohort study in an acute care university hospital in London, Ontario, Canada, involving 75 patients over age 65, admitted to the general internal medicine clinical teaching units (CTU).
Measurements
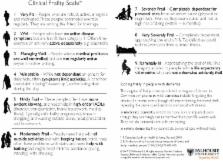
Patient demographics were collected through chart review, and CFS score was assigned to each patient after brief clinician assessment. The CFS ranges from 1 (very fit) to 9 (terminally ill) based on descriptors and pictographs of activity and functional status. The CFS was collapsed into three categories: non-frail (CFS 1–4), mild-to-moderately frail (CFS 5–6), and severely frail (CFS 7–8). Outcomes of length of stay and 90-day readmission were gathered through the LHSC electronic patient record.
Results
Severe frailty was associated with longer lengths of stay (Mean = 12.6 ± 12.7 days) compared to mild-to-moderate frailty (mean = 11.2 ± 10.8 days), and non-frailty (mean = 4.1 ± 2.1 days, p = .014). This finding was significant after adjusting for age, sex, and number of medications. Participants with higher frailty scores showed higher readmission rates when compared with those with no frailty (31.2% for severely frail, vs. 34.2% for mild-to-moderately frail vs. 19% for non-frail) although there was no significant difference in the adjusted analysis.
Conclusion
The CFS helped identify patients that are more likely to have prolonged hospital stays on the acute medical ward. The CFS is an easy to use tool which can detect older adults at high risk of complicated course and longer stay. Objective early identification of seniors with frailty in acute care units can help to target interventions to prevent complications and to implement effective discharge planning in high risk older adults.
Related collections
Most cited references17
- Record: found
- Abstract: found
- Article: not found
The frailty phenotype and the frailty index: different instruments for different purposes.
- Record: found
- Abstract: found
- Article: not found
Change in disability after hospitalization or restricted activity in older persons.
- Record: found
- Abstract: found
- Article: not found