- Record: found
- Abstract: found
- Article: found
Mapping the Minnesota living with heart failure questionnaire (MLHFQ) to EQ-5D-5L in patients with heart failure
Read this article at
Abstract
Background
Mapping algorithms can be used to convert scores from a non-preference based instrument to health state utilities. The objective of this study was to develop mapping algorithms which will enable the Minnesota Living with Heart Failure Questionnaire (MLHFQ) scores to be converted into EQ-5D-5L utility scores that can be used in heart failure related cost utility studies.
Method
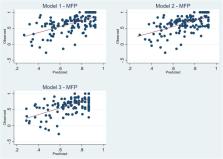
Patients diagnosed with heart failure were recruited from Australia. Mapping algorithms were developed using both direct and indirect response mapping approach. Three model specifications were considered to predict the EQ-5D-5 L utility score using MLHFQ total score (Model 1), MLHFQ domain scores (Model 2), or MLHFQ item scores (Model 3). Six regression techniques, each of which has the capability to cope with either skewness, heteroscedasticity, ceiling effects and/or the potential presence of outliers in the data set were used to identify the optimal mapping functions for each of the three models. Goodness-of-fit of the models were assessed using six indicators. In the absence of an external validation dataset, predictive performance of was assessed using three-fold cross validation method. In the indirect response mapping, EQ. 5D 5 L responses were predicted separately using the MLHFQ item scores using ordered logit model.
Results
A total of 141 patients participated in the study. The lowest mean absolute error (MAE) was recorded from the multivariable fractional polynomials (MFP) model in all three-model specifications. Regarding the indirect response mapping, results showed that the performance was comparable with the direct mapping approach based on root mean squared error (RMSE) but was worse based on MAE.
Related collections
Most cited references35
- Record: found
- Abstract: found
- Article: not found
Heart failure: preventing disease and death worldwide

- Record: found
- Abstract: found
- Article: found
Health-related quality of life measured using the EQ-5D–5L: South Australian population norms
- Record: found
- Abstract: found
- Article: not found