- Record: found
- Abstract: found
- Article: not found
Post-discharge persistent symptoms and health-related quality of life after hospitalization for COVID-19
letter
Eve Garrigues
1 ,
Paul Janvier
2 ,
Yousra Kherabi
1 ,
Audrey Le Bot
1 ,
Antoine Hamon
1 ,
Hélène Gouze
1 ,
Lucile Doucet
1 ,
Sabryne Berkani
1 ,
Emma Oliosi
1 ,
Elise Mallard
1 ,
Félix Corre
1 ,
Virginie Zarrouk
1 ,
Jean-Denis Moyer
3 ,
Adrien Galy
1 ,
Vasco Honsel
1 ,
Bruno Fantin
1 ,
Yann Nguyen
1
,
4
,
*
25 August 2020
Read this article at

There is no author summary for this article yet. Authors can add summaries to their articles on ScienceOpen to make them more accessible to a non-specialist audience.
Abstract
Dear editor,
In this journal, we recently reported a series of 279 hospitalized patients with novel
coronavirus 2019 disease (COVID-19) and their short-term outcome.
1
However, only a few studies have assessed post-discharge persistent symptoms and health-related
quality of life (HRQoL) after hospitalization for COVID-19.
2
,
3
Here, we describe a single-centre study assessing post-discharge persistent symptoms
and HRQoL of patients hospitalized in our COVID-19 ward unit more than 100 days after
their admission. COVID-19 diagnosis was based on positive SARS-CoV-2 real-time reverse
transcriptase-polymerase chain reaction on nasal swabs, and/or typical abnormalities
on chest computed tomography. Patients who were directly admitted to the ICU without
being hospitalized in our COVID-19 unit were excluded. Demographic and clinical data
at admission were extracted from electronic medical records.
We designed a short phone questionnaire to collect post-discharge clinical symptoms,
modified Medical Research Council (mMRC) dyspnoea scale scores, professional and physical
activities, and attention, memory and/or sleep disorders. HRQoL was assessed using
the EQ-5D-5L questionnaire, a widely used, validated European questionnaire
4
. Patients are asked to rate their health state from 1 to 5 in five domains (mobility,
self-care, usual activities, pain/discomfort, and anxiety/depression) and on a scale
ranging from 0 (“the worst possible health”) to 100 (“the best possible health”) on
a visual analogue scale (EQ-VAS). Based on the answers, an EQ-5D- index can be calculated,
ranging from states worse than dead (<0) to 1 (full health).
5
All eligible patients were contacted by phone by trained physicians and were asked
to answer to the questionnaire. Deceased, unreachable, demented, bedridden and non-French
speaking patients were excluded. We compared patients managed in hospital ward without
needing intensive care (“ward group”) with those who were transferred in intensive
care units (ICU) for artificial ventilation, including non-invasive ventilation, high
flow nasal cannula and/or mechanical ventilation (ICU group), with t-tests for quantitative
variables and Chi-square tests for qualitative variables. All tests were two-sided,
and a P-value <0.05 was considered statistically significant. All analyses were performed
with R version 3.6.1. (R Foundation for Statistical Computing, Vienna, Austria). The
study was approved by the local institutional review board (IRB 00006477).
Of the 279 hospitalized patients between March 15th and April 14th, 2020 in our COVID-19
unit, 48 were admitted to ICU, and 57 patients died within the three months following
admission (43 in the ward group and 14 in the ICU group) (Supplementary figure 1).
After having excluded demented or bedridden (n=18), unreachable (n=69), non-French
speaking patients (n=12), and those declining participation (n=2), 120 patients answered
the phone questionnaire after a mean (±SD) of 110.9 (±11.1) days following admission:
96 in the ward group and 24 in the ICU group for artificial ventilation (mechanical
ventilation for 14, CPAP for 10 and high flow nasal cannula for 7).
After a mean of 110.9 days, the most frequently reported persistent symptoms were
fatigue (55%), dyspnoea (42%), loss of memory (34%), concentration and sleep disorders
(28% and 30.8%, respectively) (Table 1
). Loss of hair was reported by 24 (20%) patients, including 20 women and 4 men. Comparisons
between ward- and ICU patients led to no statistically significant differences regarding
those symptoms. Thirty-five (29%) patients had a mMRC grade ≥2 (“Walks slower than
people of the same age because of dyspnoea or has to stop for breath when walking
at own pace”).
Table 1
Post-discharge persistent symptoms and health-related quality of life of 120 patients
after a mean of 110.9 days after their admission for COVID-19.
Table 1
Overall
Ward patients
ICU patients
P value
N=120
N=96
N=24
Age, years
63.2 (15.7)
64.1 (16.1)
59.6 (13.7)
0.208
Sex, male
75 (62.5)
56 (58.3)
19 (79.2)
0.099
Comorbidities
Diabetes
26 (21.7)
22 (22.9)
4 (16.7)
0.698
Hypertension
56 (46.7)
45 (46.9)
11 (45.8)
1.000
Body mass index (kg/m²)
<0.001
<25, n (%)
35 (29.2)
32 (33.3)
3 (12.5)
≥25, n (%)
57 (47.5)
37 (38.5)
20 (83.3)
Missing, n (%)
28 (23.3)
27 (28.1)
1 (4.2)
Clinical features at admission
Confusion
7 (5.8)
6 (6.2)
1 (4.2)
1.000
Cough
87 (72.5)
69 (71.9)
18 (75.0)
0.959
Dyspnoea
88 (73.3)
68 (70.8)
20 (83.3)
0.327
Myalgia
19 (15.8)
16 (16.7)
3 (12.5)
0.851
Diarrhoea
29 (24.2)
25 (26.0)
4 (16.7)
0.488
Admission data
Length of stay in hospital, days
11.2 (13.4)
7.4 (5.4)
26.5 (22.3)
<0.001
Length of stay in ICU, days
-
-
17.1 (15.7)
-
Persistent symptoms
Cough
20 (16.7)
14 (14.6)
6 (25.0)
0.358
Chest pain
13 (10.8)
11 (11.5)
2 (8.3)
0.941
Fatigue
66 (55.0)
52 (54.2)
14 (58.3)
0.891
Dyspnoea
50 (41.7)
38 (39.6)
12 (50.0)
0.487
Ageusia
13 (10.8)
9 (9.4)
4 (16.7)
0.509
Anosmia
16 (13.3)
14 (14.6)
2 (8.3)
0.638
Hair loss
24 (20.0)
18 (18.8)
6 (25.0)
0.690
Attention disorder
32 (26.7)
28 (29.2)
4 (16.7)
0.327
Memory loss
41 (34.2)
36 (37.5)
5 (20.8)
0.194
Sleep disorder
37 (30.8)
29 (30.2)
8 (33.3)
0.535
mMRC dyspnoea scale
0.438
Grade 0
56 (46.7)
47 (49.0)
9 (37.5)
Grade 1
29 (24.2)
22 (22.9)
7 (29.2)
Grade 2 or more
35 (29.2)
27 (28.1)
8 (33.3)
Professional and physical activities
Returned to work/worked before hospitalization
38/56 (67.9)
31/41 (75.6)
7/15 (46.7)
0.061
Resumed sport/practiced sport regularly before hospitalization
28/39 (71.8)
23/31 (74.2)
5/8 (62.5)
0.937
EQ-5D-5L
EQ-VAS (%)
70.3 (21.5)
69.9 (21.4)
71.7 (22.2)
0.711
EQ-5D index
0.86 (0.20)
0.86 (0.19)
0.82 (0.21)
0.306
Results are expressed as count (%) for categorical variables and as mean (standard
deviation) for quantitative variables. ICU: intensive care unit; mMRC: modified Medical
Research Council;
Before COVID-19 infection, 56 (46.7%) were active workers. Among them, 38 (69.1%)
had gone back to work at the time of the phone interview. Among the 39 patients who
had regular sports activity before their hospitalizations for COVID-19, 28 (71.8%)
have been able to resume physical activity, but at a lower level for 18 (46%). There
was no statistically significant difference between ward and ICU groups, but there
was a non-significant trend towards a reduced proportion of patients returning to
work among ICU patients (46.7% versus 77.5%, P=0.061).
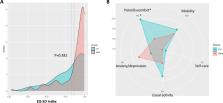
In both group, dimensions of the EQ-5D (mobility, self-care, pain, anxiety or depression,
usual activity) were altered with a slight difference in pain in the ICU group, but
no statistically significant difference in the other groups (Figure 1
). Mean EQ-VAS was 70.3% and mean EQ-5D index 0.86, with no difference between ICU
and ward patients (Table 1).
Figure 1
Health-related quality of life after hospitalization for COVID-19 assessed by the
EQ-5D 5L in the ward and the ICU groups. 1A: Distribution of the EQ-5D index (0: death
to 1: full health). 1B: EQ-5D 5L scores in the ward and in the ICU groups on each
domain. Each domain is scored on a 5-point scale: 1 no problem, 2 slight problem,
3 moderate problem, 4 severe problem, 5 unable to do. *: P=0.032.
Figure 1
The present study shows that most patients requiring hospitalization for COVID-19
still have persistent symptoms, even 110 days after being discharged, especially fatigue
and dyspnoea. These results highlight the need for a long-term follow-up of those
patients and rehabilitation programs. Surprisingly, many patients (mainly women) spontaneously
reported significant hair loss, which may correspond to a telogen effluvium, secondary
to viral infection and/or a stress generated by the hospitalization and the disease.
6
Nevertheless, HRQoL was quite satisfactory, as most patients who had a professional
activity before the infection went back to work.
Except pain or discomfort, we found no significant difference regarding persistent
symptoms and HRQoL between ward patients versus ICU patients. This clearly supports
the interest of a full resuscitation for COVID patients despite heaviness of cares.
However, patients from our “ICU group” were relatively non-severe, as those who were
directly admitted to ICU (thus corresponding to the most severe forms) were not included
in our study.
Other limitations of our study include the limited number of patients, the single-centre
nature of our series, and the high rate of unreachable patients, which could lead
to differential bias.
In conclusion, many symptoms persist several months after hospitalization for COVID-19.
While there were few differences between HRQoL between ward and ICU patients, our
findings must be confirmed in larger cohorts, including more severe ICU patients.
AUTHOR CONTRIBUTIONS
All authors have made substantial contributions to this work and have approved the
final version of the manuscript. Concept and design: EG, BF, YN. Acquisition of data:
all authors. Statistical analysis: YN. Interpretation of data: EG, BF, YN. Writing
original draft: EG, YN. Writing review and editing: all authors.
FINANCIAL SUPPORT
None
Declaration of Competing Interest
None of the authors declared any competing interest in link with the present study.
Related collections
Most cited references4
- Record: found
- Abstract: found
- Article: found
Persistent Symptoms in Patients After Acute COVID-19
Angelo Carfì, Roberto Bernabei, Francesco Landi (2020)
- Record: found
- Abstract: found
- Article: found
Post‐discharge symptoms and rehabilitation needs in survivors of COVID‐19 infection: a cross‐sectional evaluation
Stephen Halpin, Claire McIvor, Gemma Whyatt … (2020)

- Record: found
- Abstract: found
- Article: found
A French Value Set for the EQ-5D-5L
Luiz Flavio Andrade, Kristina Ludwig, Juan Goñi … (2020)