- Record: found
- Abstract: found
- Article: found
Zika Virus Infection as a Cause of Congenital Brain Abnormalities and Guillain–Barré Syndrome: Systematic Review
Read this article at
Abstract
Background
The World Health Organization (WHO) stated in March 2016 that there was scientific consensus that the mosquito-borne Zika virus was a cause of the neurological disorder Guillain–Barré syndrome (GBS) and of microcephaly and other congenital brain abnormalities based on rapid evidence assessments. Decisions about causality require systematic assessment to guide public health actions. The objectives of this study were to update and reassess the evidence for causality through a rapid and systematic review about links between Zika virus infection and (a) congenital brain abnormalities, including microcephaly, in the foetuses and offspring of pregnant women and (b) GBS in any population, and to describe the process and outcomes of an expert assessment of the evidence about causality.
Methods and Findings
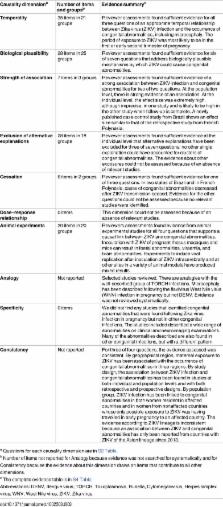
The study had three linked components. First, in February 2016, we developed a causality framework that defined questions about the relationship between Zika virus infection and each of the two clinical outcomes in ten dimensions: temporality, biological plausibility, strength of association, alternative explanations, cessation, dose–response relationship, animal experiments, analogy, specificity, and consistency. Second, we did a systematic review (protocol number CRD42016036693). We searched multiple online sources up to May 30, 2016 to find studies that directly addressed either outcome and any causality dimension, used methods to expedite study selection, data extraction, and quality assessment, and summarised evidence descriptively. Third, WHO convened a multidisciplinary panel of experts who assessed the review findings and reached consensus statements to update the WHO position on causality. We found 1,091 unique items up to May 30, 2016. For congenital brain abnormalities, including microcephaly, we included 72 items; for eight of ten causality dimensions (all except dose–response relationship and specificity), we found that more than half the relevant studies supported a causal association with Zika virus infection. For GBS, we included 36 items, of which more than half the relevant studies supported a causal association in seven of ten dimensions (all except dose–response relationship, specificity, and animal experimental evidence). Articles identified nonsystematically from May 30 to July 29, 2016 strengthened the review findings. The expert panel concluded that (a) the most likely explanation of available evidence from outbreaks of Zika virus infection and clusters of microcephaly is that Zika virus infection during pregnancy is a cause of congenital brain abnormalities including microcephaly, and (b) the most likely explanation of available evidence from outbreaks of Zika virus infection and GBS is that Zika virus infection is a trigger of GBS. The expert panel recognised that Zika virus alone may not be sufficient to cause either congenital brain abnormalities or GBS but agreed that the evidence was sufficient to recommend increased public health measures. Weaknesses are the limited assessment of the role of dengue virus and other possible cofactors, the small number of comparative epidemiological studies, and the difficulty in keeping the review up to date with the pace of publication of new research.
Conclusions
Rapid and systematic reviews with frequent updating and open dissemination are now needed both for appraisal of the evidence about Zika virus infection and for the next public health threats that will emerge. This systematic review found sufficient evidence to say that Zika virus is a cause of congenital abnormalities and is a trigger of GBS.
Abstract
In a systematic review, Nicola Low and colleagues use a causality framework to examine the evidence for zika virus infection as a cause of congenital brain abnormalities and Guillain–Barré syndrome.
Author Summary
Why Was This Study Done?
-
In 2015, the mosquito-borne Zika virus caused epidemics of a mild viral illness for the first time in Brazil and then other countries in Latin America and the Caribbean.
-
In mid to late 2015, clinicians in northeastern Brazil reported unexpected increases in the numbers of babies born with abnormally small heads (microcephaly) and of adults with Guillain–Barré syndrome (GBS), a paralytic condition triggered by certain infections.
-
In February 2016, the World Health Organization (WHO) declared a Public Health Emergency of International Concern and called for research about the causal relationship between Zika virus and congenital brain abnormalities, including microcephaly, and GBS.
What Did the Researchers Do and Find?
-
We developed a causality framework for Zika virus and (a) congenital brain abnormalities, and (b) GBS. For each outcome, we developed specific questions in ten different dimensions of causality: temporality; biological plausibility; strength of association; exclusion of alternative explanations; cessation; dose–response relationship; animal experimental evidence; analogy; specificity; and consistency of findings.
-
We did a systematic review of published and unpublished evidence up to May 30, 2016. We summarised the evidence descriptively. A panel of experts assessed the findings and reached a consensus about causality.
-
For congenital brain abnormalities, we assessed 72 studies that addressed questions in one or more causality dimensions. Reports of pregnancies affected by Zika virus have come from countries with circulating Zika virus in the Americas, the Pacific region, and West Africa. Clinical reports have documented Zika virus infection in pregnant women followed by foetal abnormalities, particularly with infection in the first trimester. These women did not have any other congenital infection or dengue virus infection. The risk of congenital brain abnormalities could be around 50 times higher in mothers who had Zika virus infection in pregnancy compared with those who did not. In laboratory studies, Zika virus has been shown to cross the placenta and replicate in human brain cells.
-
For GBS, we assessed 36 studies that addressed questions about one or more causality dimensions. In several countries in the Americas and the Pacific region, a temporal association has been found, with symptoms of Zika virus infection preceding the onset of GBS. In these countries, surveillance reports of cases of GBS followed the pattern of reports of Zika-like illness. During a Zika virus outbreak in French Polynesia in 2013–14, scientists estimated that around one in 4000 people with Zika virus infection developed GBS. The odds of having had a recent Zika virus infection were more than 30 times higher in patients with GBS than those without in a hospital-based study in French Polynesia. Several other infections that can trigger GBS were excluded.
Related collections
Most cited references63
- Record: found
- Abstract: found
- Article: not found
Causation and causal inference in epidemiology.
- Record: found
- Abstract: not found
- Article: not found
Zika virus in Brazil and macular atrophy in a child with microcephaly.
- Record: found
- Abstract: found
- Article: not found