- Record: found
- Abstract: found
- Article: not found
A RAPID SYSTEMATIC REVIEW OF THE EFFICACY OF FACE MASKS AND RESPIRATORS AGAINST CORONAVIRUSES AND OTHER RESPIRATORY TRANSMISSIBLE VIRUSES FOR THE COMMUNITY, HEALTHCARE WORKERS AND SICK PATIENTS
Read this article at

Abstract
Background
The pandemic of COVID-19 is growing, and a shortage of masks and respirators has been reported globally. Policies of health organizations for healthcare workers are inconsistent, with a change in policy in the US for universal face mask use. The aim of this study was to review the evidence around the efficacy of masks and respirators for healthcare workers, sick patients and the general public.
Methods
A systematic review of randomized controlled clinical trials on use of respiratory protection by healthcare workers, sick patients and community members was conducted. Articles were searched on Medline and Embase using key search terms.
Results
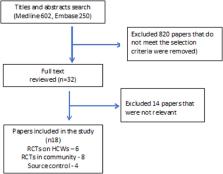
A total of 19 randomised controlled trials were included in this study – 8 in community settings, 6 in healthcare settings and 5 as source control. Most of these randomised controlled trials used different interventions and outcome measures. In the community, masks appeared to be more effective than hand hygiene alone, and both together are more protective. Randomised controlled trials in health care workers showed that respirators, if worn continually during a shift, were effective but not if worn intermittently. Medical masks were not effective, and cloth masks even less effective. When used by sick patients randomised controlled trials suggested protection of well contacts.
Conclusion
The study suggests that community mask use by well people could be beneficial, particularly for COVID-19, where transmission may be pre-symptomatic. The studies of masks as source control also suggest a benefit, and may be important during the COVID-19 pandemic in universal community face mask use as well as in health care settings. Trials in healthcare workers support the use of respirators continuously during a shift. This may prevent health worker infections and deaths from COVID-19, as aerosolisation in the hospital setting has been documented.
Related collections
Most cited references33
- Record: found
- Abstract: found
- Article: not found
Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: a descriptive study
- Record: found
- Abstract: found
- Article: not found
Aerosol and Surface Stability of SARS-CoV-2 as Compared with SARS-CoV-1
- Record: found
- Abstract: found
- Article: not found