- Record: found
- Abstract: found
- Article: found
Backtable ureteroscopy for retrieval of retained stent or stone: A novel technique in renal autotransplant
case-report
28 January 2018
Read this article at
There is no author summary for this article yet. Authors can add summaries to their articles on ScienceOpen to make them more accessible to a non-specialist audience.
Abstract
1
Introduction
Loin pain hematuria syndrome (LPHS), first described in 1967, is a disorder of chronic,
severe flank pain without an identifiable source. Patients suffer from extreme unilateral
or bilateral flank pain accompanied by microscopic or gross hematuria.
1
The etiology behind this syndrome remains unclear. Pathophysiologic mechanisms of
LPHS include immune hypersensitivity, abnormal glomerular basement membrane thickening,
somatization, abnormal ureteral peristalsis, intratubular calcium deposition, and
nephritis; however, the diagnosis of LPHS remains a diagnosis of exclusion.
2
Diagnostic criteria include characteristic renal pain present for at least 6 months
requiring substantial opioid therapy as treatment, hematuria present in multiple urinalyses,
and lack of other etiology of symptoms. Evaluation often includes urinalysis, renal
ultrasound, abdominal CT scan, and renal biopsy.
1
Despite multiple proposed interventions, many patients suffer from this pain for years,
requiring chronic use of opioids, before ultimately receiving curative treatment.
Medical therapies including analgesics and ACE inhibitors are sometimes able to provide
patients adequate symptom relief. Other minimally invasive therapies such as intraureteric
capsaicin injection and ureteric bupivacaine infusion have shown mixed results.
3
Non-invasive or minimally invasive therapies should be attempted primarily as patients
with LPHS do not suffer long term decline in renal function and up to 30% of patients
will have spontaneous resolution of their symptoms. In patients with persistent symptoms
despite trials of medical therapy, surgical options for LPHS should be considered.
Surgical options consist of renal denervation, nephrectomy, and renal autotransplantation.
Renal denervation has only a 27% rate cure for patients with LPHS. Renal autotransplantation,
first described in 1985, holds the promise of cure and making chronic pain patients
“changed people” within only a couple weeks from surgery.
4
Renal autotransplantation is a safe procedure which can provide pain improvement in
90% of patients.
Nineteen patients have undergone renal autotransplantation at the University of Utah
over the past 3 years. Of these patients, two had intra-renal objects present at the
time of surgery. One had a retained nephrostomy tube fragment at the time of transplantation
and another had a renal stone. Both patients underwent laparoscopic hand-assisted
nephrectomy. This paper describes one case in which “backtable ureteroscopy” was used
to remove the retained object prior to autotransplantation (Fig. 1).
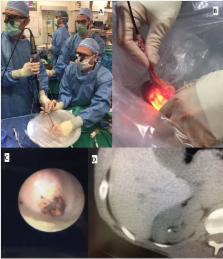
Fig. 1
Legend: A: Backtable ureteroscopy of an explanted kidney. B: External view of ureteroscope
within renal graft. C: Kidney stone as seen on ureteroscopy. D: Kidney stone as seen
on CT.
Fig. 1
2
Case report
A previously healthy 34 year old female was referred for chronic loin pain hematuria
syndrome. She initially noticed severe right flank pain in 2003 and suffered from
this pain since that time despite multiple attempted interventions. Prior to referral,
she had seen multiple physicians, including urologists, who were unable to find a
solution for her pain. Her kidney appeared normal without renal dysfunction. The only
abnormality was a small, right upper pole kidney stone which had not passed for multiple
years. While the stone was not positioned in a location that caused obstruction or
one that typically causes severe pain. She had classic symptoms of obstructed nephrolithiasis.
After years of suffering, she was diagnosed with loin pain hematuria syndrome. Her
chronic pain could no longer be attributed to the kidney stone alone. At this point,
we discussed the option of right renal autotransplant. She had been considering the
option of nephrectomy alone and was eager to undergo this procedure because it would
preserve her renal function. Prior to her operation, she underwent renal hilar block
with interventional radiology. She had a complete reduction in her pain after injection,
which returned approximately 24 hours later when the block had worn off.
Pre-operative imaging demonstrated normal renal anatomy with a single artery, vein,
and ureter. The renal stone was again visualized. The kidney was explanted with a
right laparoscopic hand-assisted nephrectomy and taken to the backtable. After flushing
the kidney with preservation solution and cooling it in an ice bath, ureteroscopy
was performed to identify and remove the retained stone (Fig. 1). The stone was retrieved
with a basket and removed successfully. The kidney was then prepared for transplant
and transplanted into the right lower quadrant in standard fashion.
The patient recovered from the procedure well and reported complete resolution of
flank pain on post-operative day 1. The transplanted kidney functioned well (creatinine
0.61) after the procedure. She was discharged from the hospital on post-operative
day 4 without complication.
3
Discussion
Renal autotransplantation is a well described procedure for treatment of renal artery
stenosis, renal artery aneurysm, and high ureteral injuries.
5
While not first line therapy, renal autotransplantation is a safe and effective treatment
modality for carefully selected patients with LPHS non-responsive to less invasive
therapies.
1
Renal autotransplant has been shown to provide long term pain relief for 70–100% of
patients with LPHS, with follow-up extending to 8 years and beyond.
1
As evidence mounts demonstrating the safety and efficacy of renal autotransplant for
LPHS, further research is required to optimize this procedure to provide the best
outcomes for patients.
To our knowledge, this is the first description of backtable ureteroscopy to remove
retained objects from the kidney prior to autotransplantation. From our limited experience,
it is a safe method to prepare kidneys for autotransplantation. Removal of retained
objects prior to autotransplantation can help protect the graft kidney by removing
potential sources of infection or encrustation and preventing obstruction, ultimately
improving graft survival. Furthermore, this procedure is technically easier than post-transplant
ureteroscopy due to the position of the vesicoureteral anastomosis high on the dome
of the bladder. While further experience with this method is required, backtable ureteroscopy
should be in the toolkit of surgeons performing renal autotransplantation.
Source of funding
None.
Conflicts of interest
No conflicts of interest exist for any of the authors.
Related collections
Most cited references4

- Record: found
- Abstract: found
- Article: found
Loin pain hematuria syndrome
Adeel S. Zubair, Hassan Salameh, Stephen Erickson … (2015)
- Record: found
- Abstract: found
- Article: not found
Renal autotransplantation for severe loin-pain/haematuria syndrome.
- Record: found
- Abstract: not found
- Article: not found
A nationwide analysis of kidney autotransplantation
Z Moghadamyeghaneh, M.H. Hanna, R Fazlalizadeh (2017)