- Record: found
- Abstract: found
- Article: found
The european primary care monitor: structure, process and outcome indicators
Read this article at
Abstract
Background
Scientific research has provided evidence on benefits of well developed primary care systems. The relevance of some of this research for the European situation is limited.
There is currently a lack of up to date comprehensive and comparable information on variation in development of primary care, and a lack of knowledge of structures and strategies conducive to strengthening primary care in Europe. The EC funded project Primary Health Care Activity Monitor for Europe (PHAMEU) aims to fill this gap by developing a Primary Care Monitoring System (PC Monitor) for application in 31 European countries. This article describes the development of the indicators of the PC Monitor, which will make it possible to create an alternative model for holistic analyses of primary care.
Methods
A systematic review of the primary care literature published between 2003 and July 2008 was carried out. This resulted in an overview of: (1) the dimensions of primary care and their relevance to outcomes at (primary) health system level; (2) essential features per dimension; (3) applied indicators to measure the features of primary care dimensions. The indicators were evaluated by the project team against criteria of relevance, precision, flexibility, and discriminating power. The resulting indicator set was evaluated on its suitability for Europe-wide comparison of primary care systems by a panel of primary care experts from various European countries (representing a variety of primary care systems).
Results
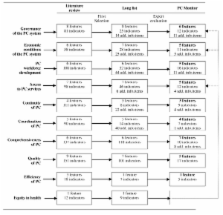
The developed PC Monitor approaches primary care in Europe as a multidimensional concept. It describes the key dimensions of primary care systems at three levels: structure, process, and outcome level. On structure level, it includes indicators for governance, economic conditions, and workforce development. On process level, indicators describe access, comprehensiveness, continuity, and coordination of primary care services. On outcome level, indicators reflect the quality, and efficiency of primary care.
Conclusions
A standardized instrument for describing and comparing primary care systems has been developed based on scientific evidence and consensus among an international panel of experts, which will be tested to all configurations of primary care in Europe, intended for producing comparable information. Widespread use of the instrument has the potential to improve the understanding of primary care delivery in different national contexts and thus to create opportunities for better decision making.
Related collections
Most cited references11

- Record: found
- Abstract: found
- Article: found
The breadth of primary care: a systematic literature review of its core dimensions
- Record: found
- Abstract: found
- Article: not found
The contribution of primary care systems to health outcomes within Organization for Economic Cooperation and Development (OECD) countries, 1970-1998.
- Record: found
- Abstract: not found
- Article: not found